The safest knee cartilage repair rehab exercises are the ones that match the phase your knee is actually in. In the first weeks, that may mean a heel slide on the bed and a quad set with your leg straight. Months later, it may mean step-ups, balance work, or low-impact cardio. Those are not interchangeable exercises. They load the repair in very different ways.
Use the timing below as orientation, not permission. Your surgeon’s protocol, the exact procedure, lesion location, swelling, pain, range of motion, and physical therapist’s assessment decide when you move forward.
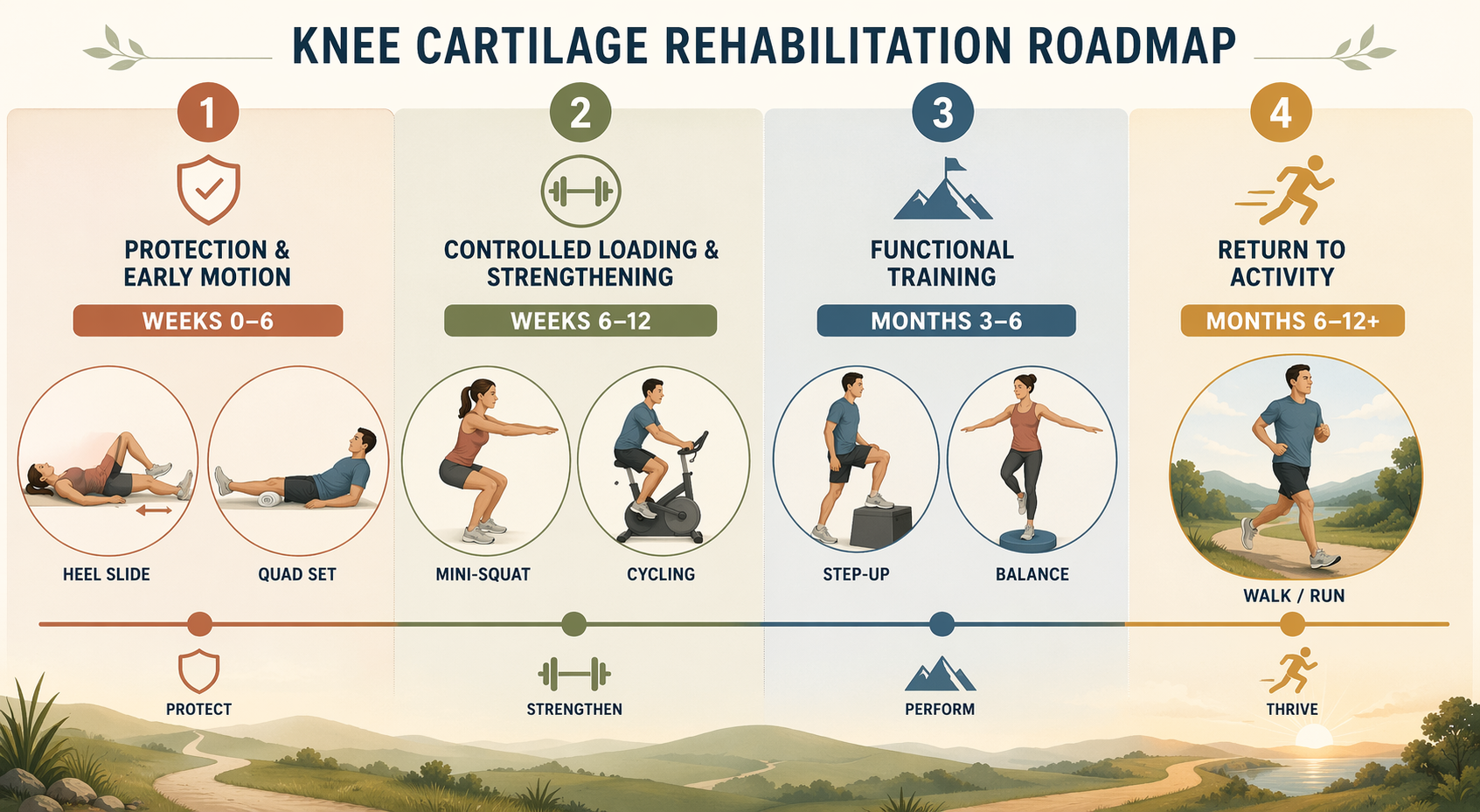
| Phase | Common Timing | Main Goal | Typical Home Exercises |
|---|---|---|---|
| Protection & Early Motion | Weeks 0-6 | Protect the repair while restoring extension and early flexion | Quad sets, heel slides, straight leg raises if cleared, ankle pumps, CPM when prescribed |
| Controlled Loading & Strengthening | Weeks 6-12 | Progress from protected weight bearing into controlled closed-chain strength | Mini-squats in limited range, leg press if prescribed, stationary cycling, pool therapy |
| Functional Training | Months 3-6 | Build usable control for stairs, walking, balance, and daily movement | Step-ups, single-leg balance, controlled lunges, swimming, elliptical, treadmill walking |
| Return to Activity | Months 6-12+ | Return to impact only after testing and clearance | Sport-specific drills, impact progression, running or jumping only when cleared |
Phase 1: Protection & Early Motion, Usually Weeks 0-6
This phase is where people often feel least athletic and have the most to protect. The goal is not to “work the knee.” The goal is to keep the knee moving enough to avoid stiffness, wake up the quadriceps, control swelling, and respect the weight-bearing limits set for the procedure.
Across orthopedic cartilage-surgery protocols, two early motion gates come up repeatedly: full knee extension within about 2 weeks and 90 degrees of flexion by about week 6.[1] Those targets matter because a knee that cannot straighten or bend early becomes harder to normalize later. They do not mean forcing motion through pain, bouncing into range, or treating the knee like a stretching project.

The early exercises are small for a reason
- Quad sets: Lie or sit with the knee straight, tighten the front thigh muscle, and hold briefly without lifting the heel. This is usually one of the first ways to restore quadriceps activation without bending or loading the knee.
- Heel slides: Slide the heel toward you only as far as your protocol allows, then return slowly. Early flexion work should feel controlled, not yanked.
- Straight leg raises: These are usually appropriate only when you can keep the knee fully straight during the lift and your clinician has cleared them. A lagging, bent-knee raise is a sign the quad is not ready.
- Ankle pumps: These keep the lower leg moving while your knee activity is limited.
- CPM use: Some microfracture protocols include continuous passive motion for 6-8 hours per day in the early phase.[1]
The procedure matters here. Microfracture commonly has stricter early weight-bearing protection, with 4-6 weeks of non-weight-bearing often used in protocols.[1] MACI protocols may allow earlier progression, but that does not make MACI a casual loading program. It means the permitted loading pattern is different and should follow the surgeon’s written plan.
At home, this phase often happens beside a bed, on a floor mat, or in a chair. That is fine. What is not fine is quietly upgrading the plan because the exercises feel too easy. If the day’s assignment is heel slides, quad sets, and protected walking with crutches, that is the work.
Phase 2: Controlled Loading & Strengthening, Usually Weeks 6-12
This is the phase where “strengthening” can become a dangerous word if it is heard as normal training. The knee may look calmer. The incisions may be healed. Daily movement may feel less dramatic. But the repair tissue is still being introduced to load, and that introduction should be gradual.
Controlled closed-chain loading often begins in this window: mini-squats in a limited 0-60 degree range, leg press if prescribed, stationary cycling, and pool therapy are common protocol exercises.[1] Weight bearing usually progresses from partial to full under physical therapy guidance. For MACI, patient rehabilitation materials describe many patients progressing to full weight bearing and getting off crutches around 8-12 weeks, but that is a typical timeline rather than a guarantee.[2]
What controlled loading looks like at home
- Mini-squats: Use a counter, chair back, or wall for support. Stay in the range your therapist gives you, often shallow at first, and keep the movement slow.
- Stationary cycling: Use low resistance and a setup that allows smooth motion. Cycling is usually about range and rhythm before conditioning.
- Leg press: If your therapist assigns it, treat the load, range, and foot position as part of the prescription. This is not the time to test strength.
- Pool walking or pool therapy: Buoyancy can reduce joint load while allowing gait practice and gentle strengthening, but entry, exit, and pool surface safety still matter.
- Gait practice: Moving from crutches to normal walking is an exercise in itself. Limping through more steps is not better than taking fewer well-controlled steps.
A useful rule in this phase is to watch the next 24 hours. More swelling, sharper pain, loss of motion, or a heavier limp after a session is information. It does not prove you failed; it tells your PT the dose may need to be adjusted.

Phase 3: Functional Training, Usually Months 3-6
By this stage, the work starts to look more like exercise, but the purpose is still specific: make the knee reliable for ordinary tasks before asking it to handle speed, impact, or fatigue. Protocol adherence during this window is described by Kerlan Jobe Institute as one of the significant factors affecting recovery success after cartilage surgery.[1]
Common exercises include step-ups, single-leg balance, controlled lunges, treadmill walking, elliptical work, swimming, and other low-impact cardio.[1] These exercises belong here only if swelling is controlled, range of motion is adequate, walking mechanics are acceptable, and the PT has cleared the progression.
- Step-ups: Start with a low step and prioritize knee alignment, slow lowering, and equal pressure through the foot.
- Single-leg balance: Begin near a counter. The goal is quiet control, not wobbling through a circus act.
- Lunges: Keep them shallow at first and use a shortened stride if your therapist allows them.
- Low-impact cardio: Swimming, elliptical training, and treadmill walking can build capacity without the same impact demands as running.
If you have already been cleared for low-impact activity and want a follow-along format, a low-impact knee-pain workout you can do at home may be useful. It should not replace your cartilage-repair protocol, especially if you are still restricted in squat depth, step height, resistance, or total volume.
Phase 4: Return to Activity, Usually Months 6-12+
Return to activity is not a date on the calendar. It is a clearance decision. High-impact exercise should wait until functional testing shows the knee can handle the task, and until the surgeon and PT agree that the repair, strength, motion, swelling response, and movement quality are ready.
Typical return-to-sport windows differ by procedure. Kerlan Jobe Institute lists microfracture return to sport around 6-9 months and MACI around 9-12 months.[1] Those ranges are not a race. A person who returns later with a quiet knee and better control is not behind someone who rushes impact and loses motion or swelling control.
This phase may include impact preparation, jogging progressions, agility drills, or sport-specific work, but those are not generic home exercises. They are tests of whether the earlier phases built enough capacity.
If You Are Managing Knee Cartilage Damage Without Surgery
Non-surgical cartilage management uses the same logic of matching exercise to tolerance, but it does not follow the same restrictions as a fresh repair. There is no graft or marrow-stimulation site to protect in the same way. The goals are usually pain control, stiffness reduction, strength, joint-friendly conditioning, and delaying or avoiding a more invasive step when appropriate.
A 2022 systematic review of 24 studies concluded that structured physical activity can have positive effects on cartilage structure and proposed a minimum 12-week program performed 3 times per week, with 60-minute sessions combining aerobic, resistance, and flexibility work.[3] That finding supports a structured conservative exercise plan; it should not be borrowed as a post-surgical timeline.
| Conservative Goal | Exercise Emphasis | How to Keep It Knee-Friendly |
|---|---|---|
| Reduce pain and stiffness | Isometric quad and hip muscle holds | Use tolerable effort and avoid positions that provoke lingering symptoms |
| Build support around the knee | Quadriceps, hamstrings, glutes, hip abductors, adductors | Progress resistance slowly and watch next-day swelling or pain |
| Improve capacity | Walking, stationary cycling, swimming | Choose low-impact work before running or jumping |
| Maintain mobility | Gentle flexibility and range-of-motion work | Do not force deep knee flexion if it increases symptoms |
The AAOS Knee Conditioning Program gives a practical model for this kind of home work: a minimum of 4-6 weeks, 4-5 days per week, with attention to the quadriceps, hamstrings, abductors, adductors, and gluteal muscles.[4] For cartilage symptoms, that muscle list matters because the knee rarely benefits from being trained as an isolated hinge while the hip stays weak.
Conservative-management studies also point toward two useful priorities: isometric exercises for pain and stiffness, and combined knee-plus-hip strengthening rather than knee strengthening alone. Those are narrower claims than saying exercise “heals cartilage.” A good home program can improve symptoms, function, and tolerance; it should not promise to reverse every cartilage defect.
Low-impact aerobic work is usually the safer starting point. Walking, stationary cycling, and swimming let you build regular activity without immediately adding jumping, pivoting, or downhill pounding. In at-risk patients, walking showed no association with structural cartilage changes over 2 years in one study, which supports keeping walking in the conversation rather than treating all loading as harmful.[5]
Progression Signs That Matter More Than Motivation
Whether you had microfracture, MACI, OATS, ACI, or no surgery at all, the question before each exercise is simple: does this belong to the current stage?
- Move from early motion to loading only when your protocol allows weight bearing and your PT is satisfied with swelling, extension, flexion, and quad control.
- Move from controlled strengthening to functional training only when walking mechanics are clean and the knee does not flare after basic loading.
- Move from functional training to impact only after functional testing and professional clearance.
- Step back or call your clinician if swelling increases, pain sharpens, range of motion decreases, or you start limping more after exercise.
Successful home rehab is not about collecting more knee exercises. It is about doing the right category of exercise at the right stage, with professional clearance whenever loading, impact, or procedure restrictions change.
References
- Recovery Guidelines After Cartilage Surgery, Kerlan Jobe Institute.
- Rehabilitation, MACI.
- Physical Activity and Knee Cartilage, Healthcare, 2022.
- Knee Conditioning Program, AAOS OrthoInfo.
- Oiestad et al. walking and structural changes study, 2015.




Comments
Join the discussion with an anonymous comment.