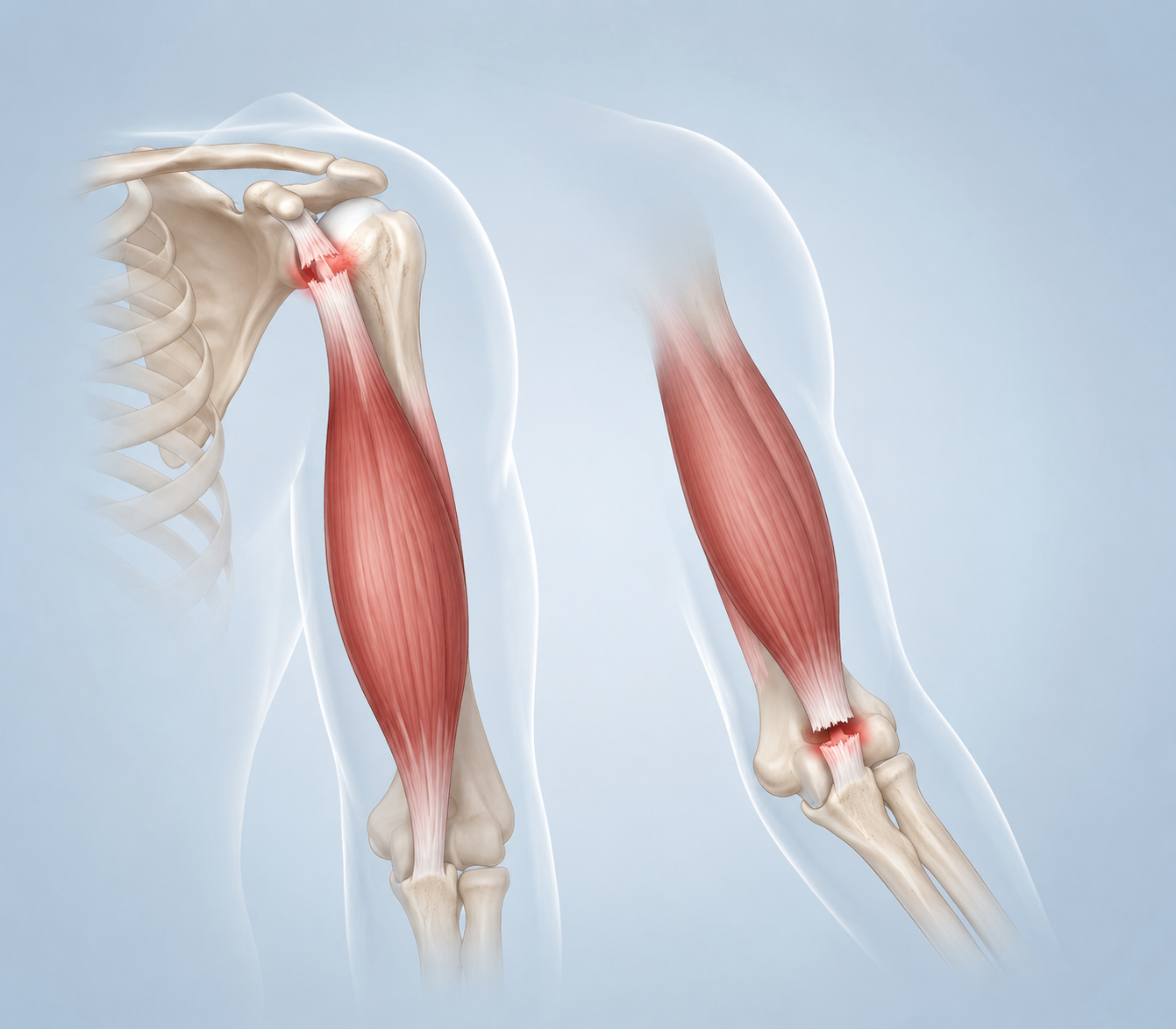
Before you pick any bicep tear recovery exercises at home, get clear on what you are recovering from. A proximal tear happens at the shoulder end of the biceps tendon. A distal tear happens at the elbow end. That difference matters more than your pain tolerance, your training history, or how badly you want to keep your routine intact.
Proximal tears are more often managed without surgery, because the other biceps tendon can help compensate in many cases; distal tears are treated much more cautiously and commonly require surgical repair or surgeon-led rehabilitation before loading begins.[1][2] A mild strain is also not the same problem as a complete rupture. UPMC describes Grade 1 biceps strains as mild injuries that may heal in weeks, Grade 2 partial tears as injuries that may take months, and Grade 3 complete tears as injuries that often need surgery.[3]
If you have a suspected distal tear, a visible deformity, major bruising, sudden weakness, a popping injury, or you cannot turn your palm upward with normal strength, do not treat this as a home-exercise problem. Get medical evaluation first. A home fitness article can help you avoid obvious mistakes, but it cannot diagnose tendon attachment or replace instructions from your surgeon or physical therapist.
The First Rule: Sharp Pain Stops the Exercise
The most useful pain rule is simple enough to remember under stress: sharp pain means stop immediately. A dull ache can show up during healing, but sharp pain, catching, sudden weakness, or pain that escalates as you continue is not a signal to push through.
That rule is especially important because many familiar upper-body exercises load the biceps tendon even when they do not look like “biceps exercises.” Pulling, curling, carrying, pressing upward, and rotating the forearm against resistance can all tug on tissue that may not be ready.
What You Can Usually Keep Training
You probably do not need to become completely inactive while the biceps heals. The safer choices are the ones that let you keep your heart, legs, and trunk working without gripping, pulling, or bracing through the injured arm.
| Usually safer while the biceps is protected | Why it is different from arm training |
|---|---|
| Walking | No direct biceps loading |
| Stationary biking | Cardio work without pulling through the arm |
| Bodyweight squats | Lower-body loading without gripping weights |
| Lunges | Lower-body training without elbow flexion resistance |
| Leg press | Machine-based leg work that does not require the injured arm to pull |
| Forearm planks | Trunk work with less direct elbow-flexion demand than hand-supported options |
| Crunches | Core work without loading the biceps tendon |
Even here, setup matters. Do not carry heavy plates, yank on bike handles, or use the injured arm to push yourself up from the floor. The exercise may be safe; the way you get into it may not be.
Exercises to Avoid Until You Are Cleared
These are not “maybe if you go light” exercises early in recovery. They directly load elbow flexion, pulling, resisted supination, pressing through the upper arm, or gripping and carrying. Singh Orthopedics and Kiritsis MD both warn against these categories after a biceps tendon tear unless a clinician has cleared them.[1][4]
- Biceps curls of any kind: dumbbell, barbell, cable, band, preacher, concentration, or hammer curls.
- Pull-ups and chin-ups: both demand strong elbow flexion and pulling through the biceps.
- Rows: dumbbell, barbell, cable, machine, and band rows all ask the biceps to assist the pull.
- Deadlifts and heavy carries: the grip and arm tension can load the injured tendon even if your legs and back feel ready.
- Bench press upward phase and overhead presses: pressing can still stress the biceps tendon during shoulder and elbow control.
The common mistake is trying to preserve strength numbers by changing the handle, angle, or tempo while keeping the same tendon demand. If the exercise still asks the injured arm to pull, curl, carry, press hard, or rotate against resistance, it has not become a recovery exercise.
A Home Progression for Mild or Clinician-Cleared Proximal Tears
The following movements are not a day-one checklist. Think of them as a progression that may fit a mild strain, a partial tear under clinical guidance, or a proximal tear being managed conservatively. If you have a distal tear, a complete tear, or post-surgical repair, use your clinician’s protocol instead.
Pendular Swings
Pendular swings are often one of the gentler ways to keep the shoulder moving without asking the biceps to contract hard. Support yourself with the uninjured arm on a table or counter, let the injured arm hang, and use your body—not the injured arm—to create small, relaxed circles or forward-back movement.
The key is passivity. If you feel yourself lifting, pulling, or actively swinging the injured arm, make the motion smaller. Stop if the movement creates sharp pain.
Elbow Flexion and Extension
When gentle elbow motion is allowed, bend and straighten the elbow without weight. Move slowly, keep the shoulder relaxed, and do not force the end range. A supported home protocol may use 2 sets of 15 repetitions, 2 times per day, but only when that motion is appropriate for your injury stage.[4]
This is range-of-motion work, not a secret curl workout. If you are trying to make it “burn,” you are doing the wrong job.
Biceps Wall Stretch
For the wall stretch, stand beside a wall, place the palm of the injured-side hand against the wall with the arm extended, and gently rotate your torso away until you feel a mild stretch through the front of the upper arm. UPMC’s biceps stretch guidance uses 15- to 30-second holds, 3 times per day.[3]

This should feel controlled and mild. Do not crank the shoulder open, bounce, or chase a deeper stretch because the arm feels tight.
Isometric Biceps Contractions
Isometrics let you create a small contraction without moving through a curl. A typical setup is to bend the elbow slightly, place the opposite hand against the injured-side forearm, and gently press as if you were beginning to curl—but without allowing movement.
Keep the effort low at first. The goal is to reintroduce tension, not test whether the tendon can tolerate your old training intensity. If the contraction produces sharp pain, stop.
Light Resisted Supination and Pronation
Supination means turning the palm upward; pronation means turning it downward. The biceps helps with supination, so this step belongs later than simple motion and stretching. When cleared, use a very light band and rotate the forearm slowly while the elbow stays close to your side.
This is one of the places where a distal tear can get into trouble fast. If the injury is at the elbow end, do not add resisted rotation because an online article made it sound like “rehab.” Wait for surgeon or physical therapist clearance.
Shoulder Flexion
Shoulder flexion means raising the arm forward. When appropriate, start without weight and keep the range comfortable. A home exercise plan may use 8 to 12 repetitions, but this belongs only in the phase where shoulder movement is allowed and does not provoke sharp pain.[4]
Do not turn shoulder flexion into a front raise with a dumbbell just because the motion feels easy. Load changes the exercise.
How Tear Grade Changes the Timeline
Grade gives you a rough recovery scale, not permission to self-diagnose. A Grade 1 strain is the category most likely to fit a short home progression. A Grade 2 partial tear can take months and deserves more supervision. A Grade 3 complete tear often moves the decision toward surgical or clinician-led care.[3]
| Injury category | What the timeline suggests | Home-exercise implication |
|---|---|---|
| Grade 1 mild strain | May heal in weeks | Gentle range of motion and careful progression may fit if symptoms stay calm |
| Grade 2 partial tear | May take months | Progression should be slower and more likely supervised |
| Grade 3 complete tear | Often needs surgery | Do not rely on a generic home plan |
For non-surgical biceps tear treatment more broadly, TSAOG Orthopedics gives a full recovery estimate of about 6 months.[5] That does not mean every mild strain takes that long, and it does not mean every complete tear can be solved without surgery. It is a useful reminder that tendon recovery is not on the same clock as muscle soreness.
Where Proximal Tears Can Be Encouraging—but Not Casual
Proximal long-head biceps ruptures are the cases where conservative care is most often discussed. Choose PT notes that physical therapy for biceps tendon rupture can include restoring motion, reducing pain, strengthening surrounding muscles, and returning gradually to activity.[2]
One IAOM-US case study followed a 49-year-old male with a complete proximal long-head biceps rupture who returned to full work duties after 9 physical therapy sessions over 3 weeks while using a home exercise program.[6] That is useful because it shows conservative recovery can work in a real proximal rupture case. It is not a promise. It is one person, one injury, one treatment course, and an unusually clean outcome.
The safe takeaway is narrower: if your tear is proximal and a clinician has ruled out a surgical problem, a progressive home program may be part of recovery. The unsafe takeaway is assuming that a fast proximal case study applies to a distal tear, a complete elbow-side rupture, or an arm that is getting weaker.
Do Not Let the Other Arm Become the Next Injury
Training around a biceps tear often turns into overusing the uninjured arm. Singh Orthopedics specifically warns about overcompensation when people favor the healthy side.[1] In a home gym, that can look like carrying everything with one hand, doing all setup one-sided, adding extra unilateral work “to make up for it,” or twisting awkwardly because the injured arm is being protected.
Protect the injured tendon, but do not punish the other shoulder, elbow, or wrist for being available. Use lighter household loads, make more trips, keep equipment setup simple, and skip exercises that require complicated one-arm bracing.
A Practical At-Home Decision Check
- If the tear may be distal, do not start resisted biceps or forearm rotation work until a clinician clears it.
- If the injury is mild or a clinician-cleared proximal tear, begin with gentle motion before stretching, isometrics, or resistance.
- If an exercise causes sharp pain, stop immediately instead of reducing the weight and trying again.
- If the exercise involves curling, pulling, rowing, heavy gripping, pressing hard, or resisted palm-up rotation, assume it is not safe until cleared.
- If you want to keep training, choose legs, walking, stationary biking, and trunk work that does not ask the injured arm to help.
For broader recovery habits after the tendon-loading restrictions are settled, a post-workout recovery routine at home can help with sleep, soreness management, and consistency. Keep that separate from the injury decision: the safest home recovery plan is still the one that respects tear type, grade, clinical clearance, and the sharp-pain stop rule.
References
- Work Out With a Biceps Tear? Dos, Don'ts & Safe Exercises, Singh Orthopedics, 2026
- Physical Therapy Guide to Biceps Tendon Rupture, Choose PT / APTA
- Biceps Strains and Tears: What to Know and How to Heal, UPMC HealthBeat, 2025
- Can I Still Workout with a Torn Bicep Tendon?, Kiritsis MD
- Bicep Tear 101, TSAOG Orthopedics, 2026
- Physical Therapy as a Conservative Treatment for a Proximal Biceps Long Head Rupture, IAOM-US, 2018




Comments
Join the discussion with an anonymous comment.